ECG Education Page
Fighting to set the pace
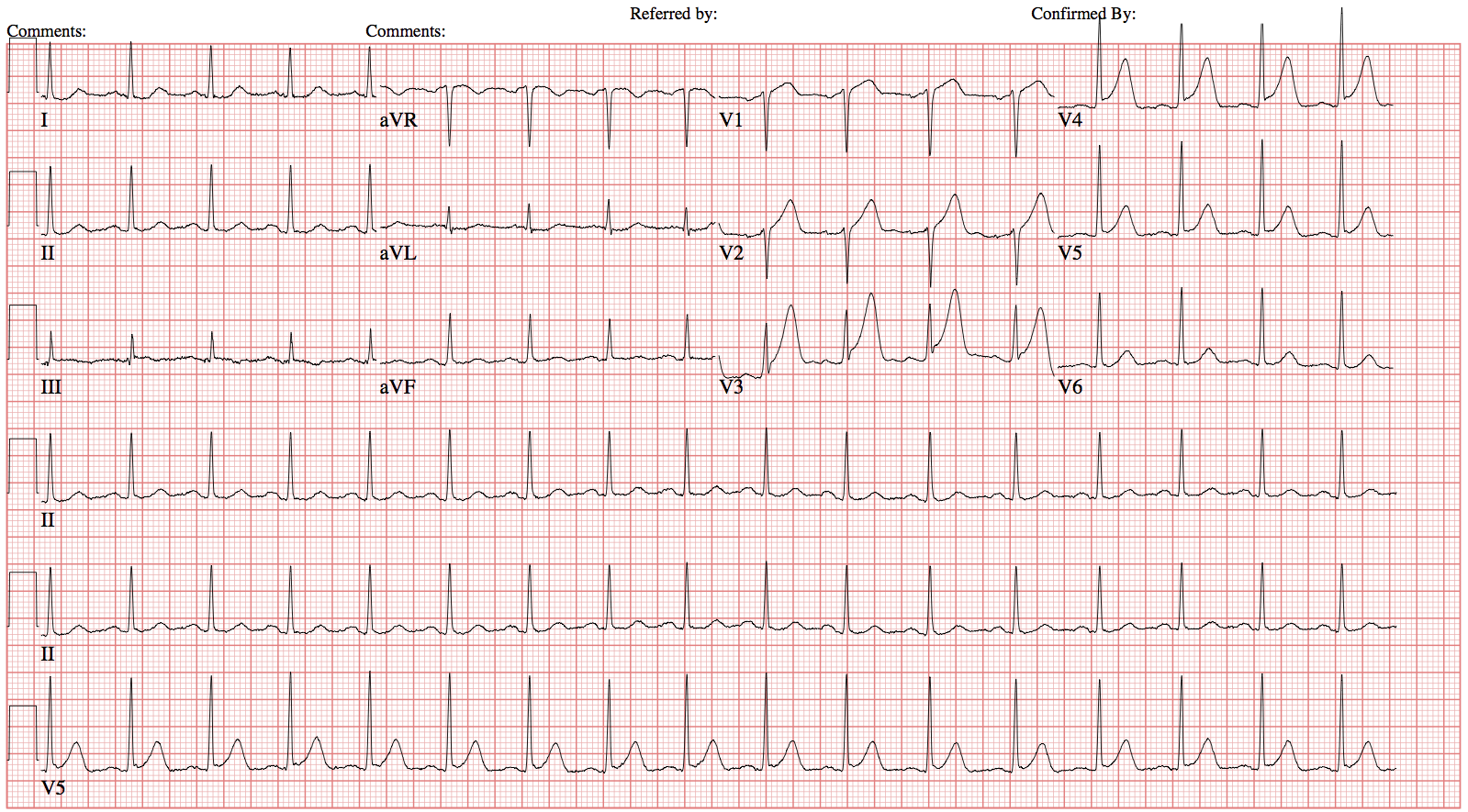
73yM with a history of atrial fibrillation on apixiban, HTN, pacemaker placement (unclear indication) who presents in transfer from outside hospital with subdural hematoma. On arrival to the ED he complains of mild headache but is otherwise asymptomatic. ECG on arrival to the ED below:

What's with the rhythm!?
Is this sinus rhythm?
Sort of...
- P before every QRS?
- Sometimes...seen best in leads II and V5, there appears to be a p wave before every narrow QRS complex
- QRS after every P?
- Yes
- P waves with similar morphology?
- Yes
Look closely at V5, what do you notice?
Prior to every p wave there appears to be a pacer spike. Therefore, approximately half the QRS complexs appear to be an atrially-paced bradycardia at a rate of ~38
Where are the wide QRS complexs coming from?
Wide QRS complexes occur regularly at a rate of ~35 which suggests a ventricular source (see table). Compexes 1, 2, 3, and 5 appear to have the same morphology and therefore are likely from a single location. QRS morphology is similar to a LBBB, so the complexes are coming from the right ventricle.
INSERT TABLE
So, what's the rhythm?
Atrially-paced bradycardia with PVCs in bigeminy v ventricular escape pacemaker
BONUS: Is the pacemaker functioning appropriately?
Answers go here
title
35 year old obese male with no known past medical history presents to the ED with chest pain. ECG on arrival to the ED is below:
Are there ST changes suggestive of ischemia?
There is 1mm ST elevation in V2, 2mm ST elevation in V3 and V4, and 1mm ST elevation in V5.
Are these ST chagnes diagnostic of STEMI in this patient?
No, for a male <40yo data-preserve-html-node="true" ST segment elevation in V2 and V3 must be >2.5mm to be considered significant. Therefore, this patient has no significant ST segment elevation in ≥ 2 contiguous leads.
INSERT TABLE BOBBY
Are these other signs of ischemia on this initial ECG?
Yes! Patient has prominent T waves in V2-4 concering for hyperacute T waves.
What are hyperacute T waves?
There is no formal accepted definition of hyperacute T waves. They are generally thought of as large T waves as compared to the QRS complex that are broad based (as opposed to hyperkalemic T waves which tend to be narrow based) with an asymetric gradual updstroke then abrupt return to baseline. They are often assocaited with J point elevation.
30 minutes later another ECG is obtained...

Are there ST changes diagnostic of STEMI now?
Yes! Patient has 1.5cm ST segment elevation in V4 and 1mm ST segment elevation in V5 diagnostic of STEMI. Although the ST segment elevation in V2 is now significant at 3mm, V3 has only 1.5mm ST segment elevation and does not technically meet criteria.
Patient was taken to the Cath Lab and was found to have 100% mid-LAD lesion that was successfully stented!
title
66yo female with a history of CAD status post stenting, diabetes, hyperension who presents with a 1 day history of lightheadedness and nausea. ECG obtained shortly after arrival is below:

Question
Answer
Question
Answer
Question
Answer
Question
Answer
Question
Answer














Quisque iaculis facilisis lacinia. Mauris euismod pellentesque tellus sit amet mollis.