Time is on Our Side
/A 79 year-man presents to your SRU by ALS squad with a report of decreased mental status. He is a resident of a nursing facility with a history of dementia, hypertension, diabetes, peripheral vascular disease, heart disease, congestive heart failure and BPH. Had enough initials? The squad reports that, according to the nursing home staff, he normally participates in self-care and can converse. He was hypotensive, tachypneic, and clammy to their assessment. Finger stick glucose was critically high. His O2 sat on room air was 86%, improving to 92% on a high-flow NRB mask.
On your assessment, the patient is obtunded, and only rolls his eyes and moans when stimulated. He coughs wetly as you examine him, but you note that his mucous membranes are extremely dry, and he feels cool to touch. His capillary refill in his hands is 3 to 4 seconds, but distal pulses are weakly palpable. His vital signs follow:
BP 86/palp, Pulse 87, RR 24 and shallow, T 95.9 F, sat 93% on 15 LPM on NRB mask.
Further exam reveals pulmonary rales, and a distended hypogastrium. His neurologic exam is non-focal, but his mental status is way below his baseline. Hydration is initiated, and he is suctioned of a large amount of thick, gooey, foul sputum. Unfortunately, the suctioning does not improve his sats...in fact they fall to 88% and persist at that level.
I stipulate that all appropriate evaluations for his presumed (and obvious) sepsis occur, as does the initiation of appropriate treatment both for the pneumonia revealed by CXR, and for the UTI and obstructive uropathy revealed on UA and ultrasound of his bladder – but this is an airway missive, so the next question asks itself: Do you want to do anything about his airway?
Apply the indications. Failing to oxygenate? Yep, and likely not quickly reversible, either. Failing to ventilate? His pCO2 on his handy VBG is 42. If you say you need an ABG to confirm this, you do not pass GO and collect $200. Protecting his airway? Right now, but you are not optimistic about his ability to do so later. Anticipated course? Rocky. He already looks exhausted, and no miracle intervention is going to readily fix that.
The need for plastic
How? Apply the Universal Algorithm... He isn’t a crash, and evaluation of his anatomical characteristics reveal him to be a favorable candidate for RSI and direct (but preferable video-augmented) laryngoscopy. Recall, that when we are confident that we can intubate from above, we should always paralyze because it optimizes the first attempt. There is minor concern because the starting point with regard to oxygenation is lower than we would like, but you can't always get what you want... and proceed with RSI. The 7 Ps are rigorously applied, and the intubation proceeds flawlessly. Touchdown dance! But wait...
During the intubation attempt, the sats fell to 88% prior to confirmation of placement by ETCO2, though the induction, paralysis, and intubation only took 90 seconds. Post intubation, strange things begin to happen...the pulse ox undergoes a glissando from the A above middle C to the A below, and the tempo of the beeps drops from that of Sympathy for the Devil to that of Wild Horses. Scarcely believing your eyes and ears, you frantically look at the pleth waveform – it correlates, and at the rise and fall of the chest – it does, and you listen to the lungs – there is good air movement. The sats continue to fall until they hit 79%. It has been an excruciatingly long 96 seconds since the tube was placed. You cast an accusatory glance at your intubating second year resident, who says, “I saw the cords! Really! Well, mostly...”. You glance at the attending... Your trembling, sweating hand reaches for the ETT and just as you are about to pull it, fearing malposition or plugging or something, the sats begin to recover. Within another minute, the sat is 96% with a great waveform. CXR confirms good placement. You mop the perspiration off of your brow and scratch your head.
Has the Pulse Ox Failed Us?
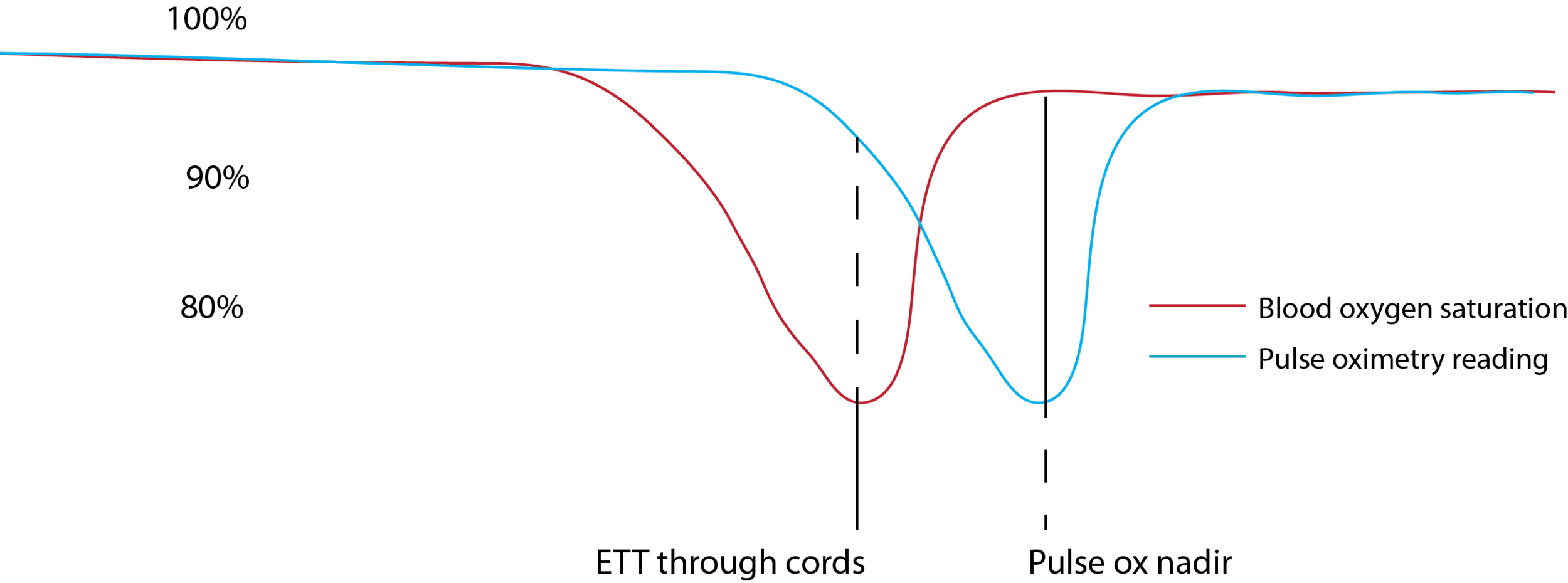
Graph displaying the false reassurance of the high pulse ox (blue) when the ETT goes through the cords, despite hypoxemia (red). Then the falsely concerningly low pulse ox nadir, although the true saturation has already recovered.
It was almost as though the pulse ox took minutes to reflect the true sat...that the patient did, in fact, desaturate prior to completion of the intubation, but you didn’t capture the degree of desaturation, or the recovery from it, until several minutes after all other indicators suggested that the tube was a righteous one. Well, guess what...the pulse ox did, in fact, take minutes to reflect the true sat. This phenomenon, variously called lag or latency, is well-recognized, but often forgotten. It has led, many times and in many places, to perfectly good ETTs and supra-glottic devices being pulled because of an over-reliance on the pulse ox and a disbelief of other confirmatory measures.
Why does this happen?
Imagine that you are a red blood cell loading up on oxygen in the pulmonary circulation with all of your buds. You pass from the pulmonary capillary circulation in to the pulmonary veins into the LA, into the LV then into the aortic root. This takes time, though not much time. Then, however, you pass with an ever-decreasing driving pressure into ever higher resistance vessels. In this particular patient, those vessels are badly narrowed by disease, and also vasoconstricted because of high sympathetic tone and cold (with rheologic consequences, as well). By the time you and a few of your compadres glide into the nailbed of his left 5th digit and start to reflect a different wavelength of light than your exhausted predecessors, minutes may have passed. Don’t be fooled by the fact that the pulse wave is almost instantly transmitted to the wrist – pressure doesn’t equal flow. Further, the software algorithms that calculate saturation in oximeters introduce some delay in a manner that varies between machines from different manufacturers.
In addition to occasionally resulting in the sacrifice of perfectly well-placed airway devices, this phenomenon has another disturbing implication: Does our “magic number” of 90% sat as the index that triggers various rescue interventions actually indicate a sat of 90%, or is the hypoxia horse already out of the barn? We have all been taught to respect this 90% threshold. Should the number be higher? Should we consider bagging at 93%? The question stands.
I.C. Cordes is written by Steven Carleton, MD PhD, Professor of Emergency Medicine at UC. Also an instructor at The Difficult Airway Course, Dr. Carleton uses I.C. Cordes to cover challenging airway cases and the use of airway equipment old and new.




