EmergencyKT Highlights: Evaluation and Treatment of Pneumonia
/Empiric antibiotics for pneumonia in the Emergency Department is complex, and the choice only gets harder when it’s 3:00 am with 15 patients in the lobby. Fear not, the Suspected Pneumonia Protocol is here to help. Here are the highlights:
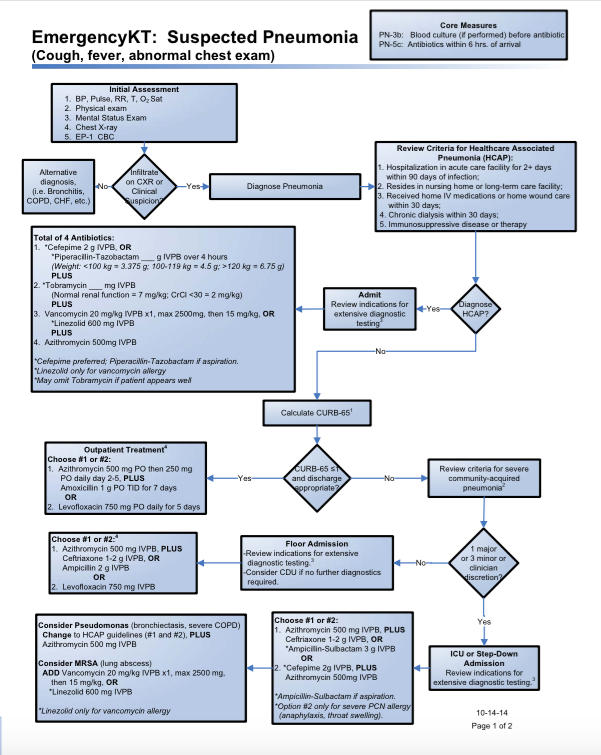
1. Does your patient have Healthcare Associated Pneumonia (HCAP)?
The full list is in the protocol, but essentially if your patient is a frequent user of healthcare, then they have HCAP. This means the pneumonia-causing microbe is more likely to be a drug-resistant one, such as Pseudomonas aeruginosa or methicillin-resistant Staphylococcus aureus. Thus, admission is a must, and you need multiple “big gun” antibiotics. However, there is a curve ball. Emergency Department patients are fundamentally different from patients who get pneumonia in the ICU. Our patients come to us from the community, so they are still at risk for the “atypicals” like Legionella pneumophila that we see in Community Acquired Pneumonia. Thus, we need four (yes, four) antibiotics: cefepime, tobramycin, vancomycin, azithromycin. The first two ensure you cover nasty multidrug-resistant gram-negatives, the third covers most gram-positives, and the last is for atypicals.


2. Does your patient look well enough for discharge?
Assuming your patient doesn’t have HCAP, if they look well (e.g. no hypoxia, no tachypnea, no hypotension) they can go home. CURB-65 is one tool available to help with this decision, but ultimately it’s up to you and your patient. Antibiotic choice is largely based on the macrolide-resistance patterns of Streptococcus pneumoniae. This is the organism most likely to cause a failure of outpatient treatment. In Cincinnati, the resistance is >25%, so monotherapy with azithromycin is a poor choice. Instead, add high-dose amoxicillin or use levofloxacin alone. Either option will cover the atypicals.
3. Just how sick is your patient?
If your patient is too sick for discharge, then you need to ask yourself how sick are they? Again, there are criteria listed in the protocol, but there is some amount of subjectivity here. If your patient is just a smidge too sick for discharge, you can still use the same outpatient antimicrobials, but switch to the IV form. However, if you’re thinking step-down or intensive care, the game changes. We need to cover some of the “odd-ball” gram-negatives, like Escherichia coli, so ceftriaxone plus azithromycin is a good choice. If your patient looks really sick (e.g. septic shock, intubated) then all bets are off. You have to start worrying about the multidrug resistant organisms we treated in HCAP, so revert to the big-gun antibiotic cocktail described above.
Keep in mind that this protocol is designed for initial antibiotic choice in the Emergency Department, not day five of admission to the intensive care unit. Also, remember that severe fungal/viral infections are always a possibility too, as pneumonia is often polymicrobial.
I hope you find this protocol useful. Happy antibiosing!
The Protocol

Many other Emergency Medicine focused evaluation and treatment protocols are available on www.emergencykt.com
References
- Mandell, L., Wunderink, R., Anzueto, A., Bartlett, J., Campbell, G., Dean, N., Dowell, S., File, T., Musher, D., Niederman, M., Torres, A., & Whitney, C. (2007) Infectious Diseases Society of America/American Thoracic Society Consensus Guidelines on the Management of Community-Acquired Pneumonia in Adults. Chest. 44 (Suppl 2) S27-S72




