Nobody Expects the Spanish Inquisition! (or, for that matter, the Cormak-Lehane Grade 4 Laryngoscopic View!)
/A 68 year-old man presents by squad with shortness of breath. He is noted to have a nearly quiet chest with very poor air movement, to be using accessory respiratory muscles, and to be slightly lethargic. Quick perusal of old records discloses a history of severe COPD, steroid and O2 dependence, HTN and ulcer disease. The squad reports that his O2 sat was 86% at the scene, improving to 92% on a NRBM and two nebs.
His vitals are: p 138, r 22 and labored, bp 156/96, O2 sat 92% on a high-flow NRBM. His POC renal returns with a pCO2 of 88. His estimated weight is about 175 lbs.
A decision is made to intubate. The assessment of airway difficulty is performed. The LEMON Law is favorable in all respects. MOANS and RODS are compromised somewhat by patient Age, and the anticipation of Stiff lungs. The SMART assessment is all favorable. The chosen method is RSI and direct laryngoscopy (DL).
The 7 Ps of RSI are skillfully followed. The patient is prepared by positioning to the sniffing position, preoxygenated by tidal breathing, and premedicated with lidocaine 1.5 mg/kg. He is induced and paralyzed using etomidate. When the R-2 takes the first look using a Mac 3 blade, they report seeing only the base of the tongue meeting the posterior pharyngeal wall. The blade is changed to a Mac 4, and the subsequent view reveals only the epiglottis meeting the posterior pharyngeal wall. The sats begin to fall, and the patient is bagged with optimal technique. The O2 sat responds to 94%.
What now?
The Unanticipated Cormack-Lehane Grade 4 (CL4) View
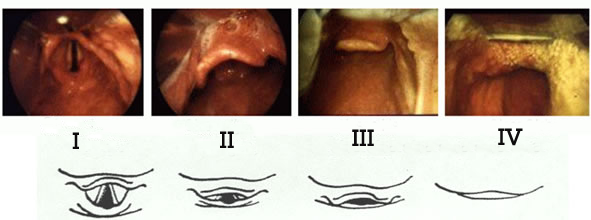
http://fibroanestesia.com/wp-content/uploads/2011/03/cormack-.png
Even in patients with a poor Mallampati score, the CL4 view is uncommon. However, in spite of doing everything right, a patient with an unanticipated, poor laryngoscopic view occurs at least monthly in our department. How can you overcome this?
1) Prevention - Choose your method of intubation wisely, based on both the patient's anatomical features, and on their respiratory status. This man was correctly assessed to have favorable anatomy…but we can only assess the epiglottis by looking at it. This reveals a limitation in the mnemonics that cannot be overcome by external exam. We simply have to live with this uncertainty. Nonetheless, RSI was a reasonable choice for this man. One could argue that his iffy sat militated for an awake method, but I think most of us would have RSI'd this guy.

2) Buy time - The patient could be anticipated to have little respiratory reserve due to his compromised respiratory starting point, and thus to tolerate apnea poorly. He also could be anticipated to respond poorly to an EGD or bagging, when his age and the compliance of his lungs were considered. In fact, he responded well to bagging…with optimal technique. This means, two hands on the mask, thenar grip, a good mask seal, an oral airway +/- a nasal trumpet in place. He was preoxygenated as well as he could be, but he had a shorter distance to skid before he fell. Remember, the fall from 100% to 90% is slow and flat, but the fall from <90% to venous sat is fast and steep. Anticipate this.
3) Diagnose the problem, and take specific action - This man was already positioned well, but positioning can slip, so reposition. Given the view, BURP/OLEM would likely not solve the problem…the issue was not that the airway was too high or anterior to see, but that the tongue and epiglottis were too posterior to permit a view of the cords. Once this diagnosis is made, the solution becomes evident; we either have to move the tongue and epiglottis out of the way (bigger Mac, or change to a Miller), get an eyeball past the tongue and epiglottis (video, optical or fiberoptic adjunct), or settle for a blind method (bougie…a VERY distant third). The order in which I listed these is no accident.
4) Deploy a toy - The change of blade size was a good idea but did not solve the problem. Change to a Miller also would be a good idea, and might have solved it, but might not have…it is worth a try. However, he required an interruption in laryngoscopy to be bagged, but responded, giving us time to think. Time to deploy an eyeball. This could be an eyeball on a blade (C-Mac or Berci-Kaplan), an eyeball on a directable wand (intubating scope), or an eyeball at the tip of the ETT (Bonfils stylet). But, to deploy an eyeball takes time. Anticipate this, and have the tools out and ready to minimize the delay. This case was solved with the C-Mac, though multiple attempts were required. My second choice would have been the Bonfils. With regard to a bougie, these have the virtue of being quick to deploy, but their intended role is to help with a partial laryngoscopic view, not an absent view.
Remember, visualizing adjuncts are not rescue devices. Because of the time required to use most of them, they are not sufficient to the task of rescuing a patient who is already crashing. The crashing patient requires either bagging or an EGD to buy time to deploy the visualizing adjunct. Among the adjuncts, the video laryngoscopes are probably the quickest to implement - if they are in the room. So prepare! I am not suggesting that we hook up all of the gadgets every time we do an intubation, but we should at least have the one(s) we would likely want for the most likely challenges that might arise, locate them, and place them within easy reach.
Update: In the interval between the original submission of this case and the present, my feelings about DL as a first step have changed. DL is, simply, inferior to VL in all respects. There may be an extraordinarily rare exception to this (excessively goopy airway), but not in the main. The Berci-Kaplan is a nice compromise to retain the skill [DL], but not harm the patient. In the near future, retaining this skill may not be sufficient justification for continuing DL in any form.
Best,
I.C.




