Antibiotic Review: Sexually Transmitted Infections
/Introduction
“Exposure to STI” is a relatively common complaint in the emergency department. Some patients are asymptomatic but fear they have been exposed and request diagnostic testing and/or treatment. Others have symptoms at the time of presentation and may or may not be aware of the fact that an STI could be causing their symptoms. Since the ED often serves patients at high risk of STIs, it is important to manage these cases appropriately in order to decrease the burden of STI infection in our surrounding populations.
The CDC has an STI Treatment Guide app for iOS and Android as well. See links below and consider adding this to your smartphone resources.
Gonorrhea and Chlamydia
In the case of a patient presenting with symptoms in the setting of a possible STI exposure, the CDC recommends point-of–care diagnostic testing and subsequent treatment. However, if this is not available, their guidelines indicate that patients should be treated empirically for gonorrhea and chlamydia while awaiting results of lab testing. [1] In the emergency department setting, a sizable group of patients may be lost to follow up which also emphasizes the importance of treatment in appropriate patients.
The antibiotic regimen we use for this today is:
Ceftriaxone 250 mg IM and azithromycin 1 g orally
Gentamicin 240 mg IM with azithromycin 2 g orally (cephalosporin allergy)
Ceftriaxone 250mg IM and doxycycline 100mg orally twice daily (azithromycin allergy)
This dual regimen was recommended by the 2010 CDC guidelines for STI treatment and continues to be recommended regardless of results of chlamydia testing in order to prevent cephalosporin resistance. [2, 3]
While it is easy to follow this treatment pathway for any patient with a chief complaint of “STI exposure,” it is also important to take a good sexual history (number of partners, previous infections, sexual activity with men/women/both, most recent HIV test) and to consider diagnostic testing and treatment for patients with symptoms of urethritis / cystitis who do not report a possible exposure. Particularly in women presenting with urethritis, data shows women are over-diagnosed with UTIs and underdiagnosed with STIs. [4] Vaginal bleeding is another chief complaint that may actually be a patient with cervicitis, consider testing in these patients as well.
A careful physical exam and history are essential when evaluating patients presenting with exposure to STI. Assess for signs of Pelvic Inflammatory Disease or tubo-ovarian abscess. Consider testing patients for HIV and syphilis if they present with high risk factors (multiple partners, concurrent drug use, multiple STIs, etc). Another consideration is multiple site testing in some symptomatic patients (e.g. rectum and pharynx). To prevent reinfection, counsel patients about having their partners evaluated and treated. Patients should also avoid sexual contact for at least one week after treatment.
Common STI Quick Hits
Trichomoniasis
Metronidazole 2 g PO, or tinidazole 2 g PO, or metronidazole 500 mg PO twice daily x 7 days.
Counsel patients to avoid alcohol when on these medication due to the disulfiram-like reaction.
Epididymitis
Ceftriaxone 250mg IM and doxycycline 100mg twice daily x 10 days (suspected to be sexually transmitted GC or CT)
Ceftriaxone 250mg IM and levofloxacin 500mg daily (will cover enteric organisms as well for men who practice insertive anal sex)
Genital Herpes Simplex
Acyclovir 400mg TID x 7-10 days for initial episode
Acyclovir 400mg TID x 5 days for episodic recurrent episodes
Syphilis
Benzathine penicillin G 2.4 million units IM single dose for primary, secondary, or latent <1 year syphilis
Benzathine penicillin G 2.4 million units IM in three doses at 1 week intervals for latent >1 year or unknown duration syphilis
Aqueous crystalline penicillin G, 18-24 million units per day, administered as 3-4 millions units IV every 4 hours or continuous infusion x 10-14 days
Lymphogranuloma venerum
Doxycycline 100mg BID x 21 days
Pediculosis Pubis
Permethrin 1% cream rinse, apply to affected area and wash off after 10 minutes
Reported Sexual Assault
For asymptomatic patients with possible exposure to STIs where health information about the other person is unknown and the patient is unlikely to follow up with testing, such as in the case of a sexual assault, the CDC guidelines are primarily geared towards women but may be extrapolated for men as well. Their recommendations include empiric antibiotic treatment for chlamydia, gonorrhea, and trichomonas, hepatitis B vaccination if the patient has not previously received this, and HPV vaccination for females 9-26 and males 9-21, or males 9-26 if they have male partners. [5] Emergency contraception should also be discussed and considered with patients.
Post Exposure Prophylaxis
Regarding PEP for HIV in these cases, the CDC recommends an individualized approach based on risk stratification. [Figure 1] Notably, PEP is not recommended if it has been over 72 hours since exposure. [5] PEP can be very expensive for patients, utilize resources to guide patients if access to medications is a barrier. For patients started on PEP, ensure they have follow up with primary care or infectious disease to monitor for side effects from medications.
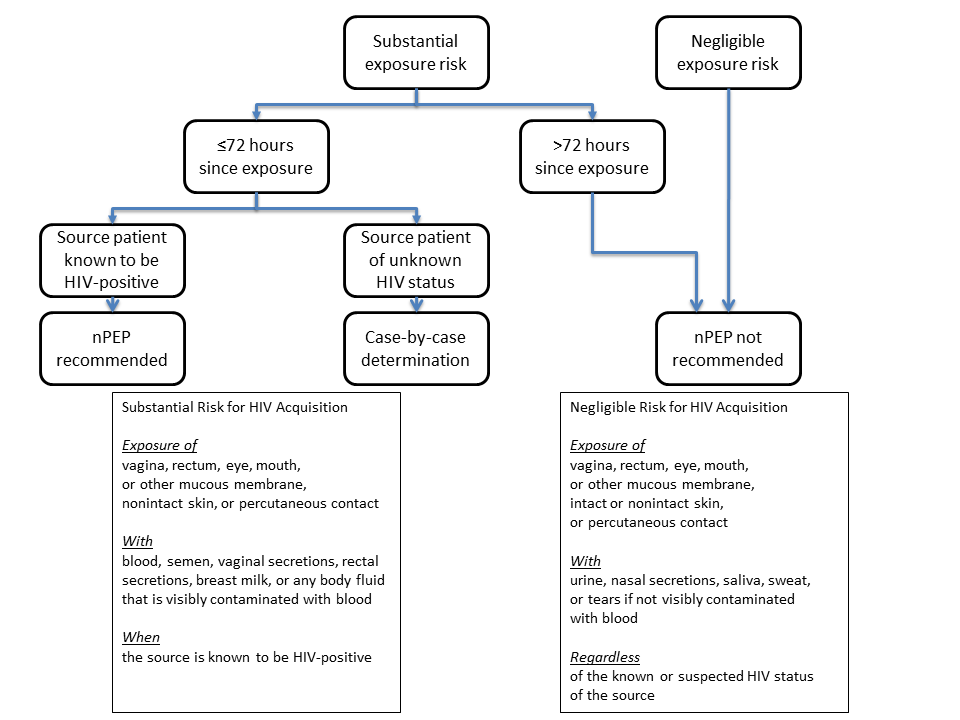
Figure 1
Sexual Assault and Abuse and STDs - 2015 STD Treatment Guidelines. 11 Jan. 2019, https://www.cdc.gov/std/tg2015/sexual-assault.htm.
Antibiotic Resistance
Usually, managing STI exposure in the emergency department is relatively straightforward. However, developing strains of antibiotic resistant bacteria, especially gonorrhea, threaten to make treatment much more complicated. Gonorrhea was not always treated with cephalosporins. Initially, gonorrhea was treated with sulfa drugs, but in the 1940s, resistance to sulfa drugs became widespread. Penicillin was then used primarily up until the mid-1980s when it too became ineffective, along with several other alternatives. At that point, fluoroquinolones such as ciprofloxacin were still effective, but by 2007, resistance to those was widespread as well.
Ceftriaxone is now the last remaining option for empirical first-line treatment. However, a gonococcus in Japan has already displayed high-level resistance to ceftriaxone, increasing the concern that gonorrhea may become untreatable in some cases in the future. [6] Further studies are needed regarding other antibiotic options, but for the time being, combination therapy with both ceftriaxone and azithromycin can at least help to delay widespread resistance of gonorrhea to ceftriaxone. [3]
AUTHOR Christa Pulvino, MD, MPH
Dr. Pulvino is a PGY-2 in Emergency Medicine at the University of Cincinnati
Post and peer editing James Li, MD
Dr. Li is a PGY-3 in Emergency Medicine at the University of Cincinnati
FACULTY EDITOR EDMOND HOOKER, MD, DrPH
Dr. Hooker is an Assistant Professor of Emergency Medicine at the University of Cincinnati and Faculty Editor of the ‘Minor Care Series’
References:
Diseases Characterized by Urethritis and Cervicitis - 2015 STD Treatment Guidelines. 11 Jan. 2019, https://www.cdc.gov/std/tg2015/urethritis-and-cervicitis.htm.
“Sexually Transmitted Diseases Treatment Guidelines, 2010.” Annals of Emergency Medicine, vol. 58, no. 1, July 2011, pp. 67–68. ScienceDirect, doi:10.1016/j.annemergmed.2011.04.006.
Bignell, C., and M. FitzGerald. “UK National Guideline for the Management of Gonorrhoea in Adults, 2011.” International Journal of STD & AIDS, vol. 22, no. 10, Oct. 2011, pp. 541–47. SAGE Journals, doi:10.1258/ijsa.2011.011267.
Tomas, Myreen E., et al. “Overdiagnosis of Urinary Tract Infection and Underdiagnosis of Sexually Transmitted Infection in Adult Women Presenting to an Emergency Department.” Journal of Clinical Microbiology, vol. 53, no. 8, Aug. 2015, pp. 2686–92. jcm.asm.org, doi:10.1128/JCM.00670-15.
Sexual Assault and Abuse and STDs - 2015 STD Treatment Guidelines. 11 Jan. 2019, https://www.cdc.gov/std/tg2015/sexual-assault.htm.
Unemo, Magnus, and William M. Shafer. “Antibiotic Resistance in Neisseria Gonorrhoeae: Origin, Evolution, and Lessons Learned for the Future.” Annals of the New York Academy of Sciences, vol. 1230, Aug. 2011, pp. E19–28. PubMed Central, doi:10.1111/j.1749-6632.2011.06215.x.




