Lessons in Transport - Upper GI Bleeding
/
It is 2am on a cold, dark, winter night and you are dispatched to a small rural hospital to transport a patient by ground with a GI bleed back to UCMC medical ICU. Enroute dispatch notifies you that your patient has deteriorated and is profoundly hypotensive. The ED physician at the outside hospital is attempting intubation for airway control. On arrival you find a middle-aged male with all the classic stigmata of end-stage liver disease. More importantly he has a systolic blood pressure of 60 and a HR of 130. A literal fountain of blood spews from the patients mouth, around a successfully placed endotracheal tube, and is now beginning to pool on the floor. You know this patient needs massive resuscitation from his likely bleeding esophageal varices... but you are 55 minutes by ground to UCMC and know that your patient will not survive the transport unless something is done to control the bleeding...
How do you control this massive bleeding?
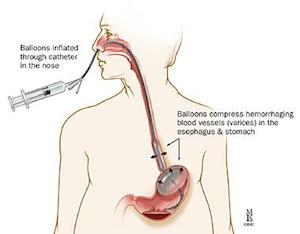
ANSWER: Placement of a Blakemore or Minnesota Tube
Indication:
Temporizing tamponade of massive gastro-esophageal bleeding that is unresponsive to medical & endoscopic therapy (or as in the case above, endoscopic therapy is unavailable)
The difference between a Sengstaken-Blakemore tube (SBT) and Minnesota Tube (MT):
SBT has 3 lumens: ports for gastric and esophageal balloons + gastric aspiration port
MT has 4 lumens: ports for gastric and esophageal balloons + gastric aspiration port + an esophageal aspiration port

Insertion Procedure:
1) Patient should be intubated first for airway protection
2) Place patient in the supine position with head of bed up at 45 degrees
3) Estimate length for tube placement from bridge of nose to xiphoid process
4) Check both balloons for leaks (holding it under ice water may stiffen the tube a bit and allow for detection of air leaks) and lubricate the tube. Be sure to fully deflate the balloons after testing.
5) Evaluate compliance curve of gastric balloon pre-insertion by inflating the ballon with incremental 100ml aliqotes of air to maximal recommended volume. (300ml for SBT and 500ml for MT) and note the corresponding balloon pressure at each step.
6) Insert via mouth (can also be inserted through the nose) by laryngoscopy into the esophagus (may need to utilize the McGill forceps)
7) Evaluate placement of gastric ballon by auscultation of the stomach and lungs with only slight inflation.
8) If possible confirm position of gastric balloon below the diaphragm and thus in the stomach on CXR.

9) Continue to inflate gastric balloon using 50ml increments. Be sure to clamp port to prevent deflation of balloon in between syringe refills. - If post insertion balloon pressure on inflation with a given volume is > 15mmHg then the pre-insertion pressure, the gastric balloon may be in the esophagus. It should be deflated and repositioned
10) Once inflated, clamp the port with 2 kelly clamps, and pull the gastric balloon back until gentle resistance is met. This should place the gastric balloon firmly against the gastric fundus.
11) Note measurement at lips (typically around 40cm) and fix securely with traction to football helmet or second ETAD tube holder. Can also attach to 1 L bag of NS hanging over an IV pull to achieve the desired 1-2 lbs of traction.
12) Tube may stretch over the next 10 minutes as it warms.
13) Suction out the stomach through the gastric aspiration port.
14) Evaluate for continued bleeding via aspiration of the esophageal port on a MT. If utilizing a SBT then you will need to place a salem-sump along side the SBT to serve as the esophageal port.
15) If bleeding persists increase tube tension by 1-2 lbs of pressure
16) If still have continued bleeding as evidenced by output of bright red blood from gastric or esophageal aspirations ports then inflate esophageal balloon. Attach a manometer to the second 3 way stopcock on the esophageal port and Do not let this pressure exceed 40 mmHg. Esophageal balloon inflation should ALWAYS be done under strict pressure monitoring as the risk of necrosis and or perforation is high.
17) Once the esophageal balloon is inflated double clamp the port with 2 kelly clamps.
Potential Complications:
Inflating the large gastric balloon in the esophagus resulting in perforation... this is usually fatal!!!
Esophageal perforation despite correctly placed balloons
Hemorrhage
Aspiration
Pain
Pressure Necrosis: should not be in place for more than 24-36 hours.
Cardiac arrhythmias
Balloon Migration resulting in acute airway obstruction
For additional resources and a fantastic video by Dr. Weingart see below. Also save the attached cheat sheet to your mobile device for quick reference
http://emcrit.org/procedures/blakemore-tube-placement/http://lifeinthefastlane.com/education/ccc/senkstaken-blackmore-and-minnesota-tubes/
Quick Reference Sheet from Dr. Weingart at www.emcrit.org:




