US - The Wall (Plot?) Thickens: Ultrasound of the Month
/THE CASE…
The patient is a young female with a past medical history of sleeve gastrectomy who initially presented to an outside hospital complaining of lightheadedness, generalized weakness, and nausea. She denied abdominal pain, diarrhea, and fevers. At the referring institution she had a full laboratory workup, which was significant for markedly elevated AST, ALT, and alkaline phosphatase, in conjunction with a mixed hyperbilirubinemia. She then had a right upper quadrant (RUQ) ultrasound which was interpreted as follows:
“Gallbladder is not significantly distended. Multiple calculi seen, largest measuring 1 cm. There is heterogeneous wall thickening measuring 1 cm and mild pericholecystic fluid. Common duct is nondilated, measuring 4.9 mm.
Impression: Gallbladder calculi with wall thickening and pericholecystic fluid worrisome for acute cholecystitis.”
The patient received 1 liter of normal saline, ciprofloxacin, metronidazole, and ondansetron prior to transfer for evaluation by acute care surgery. In our emergency department (ED) the patient reported that her pre-syncopal symptoms had resolved and she was otherwise feeling well. She continued to deny abdominal pain. Her physical exam was unremarkable. We performed a bedside RUQ ultrasound.
AND NOW FOR THE ULTRASOUND IMAGES…
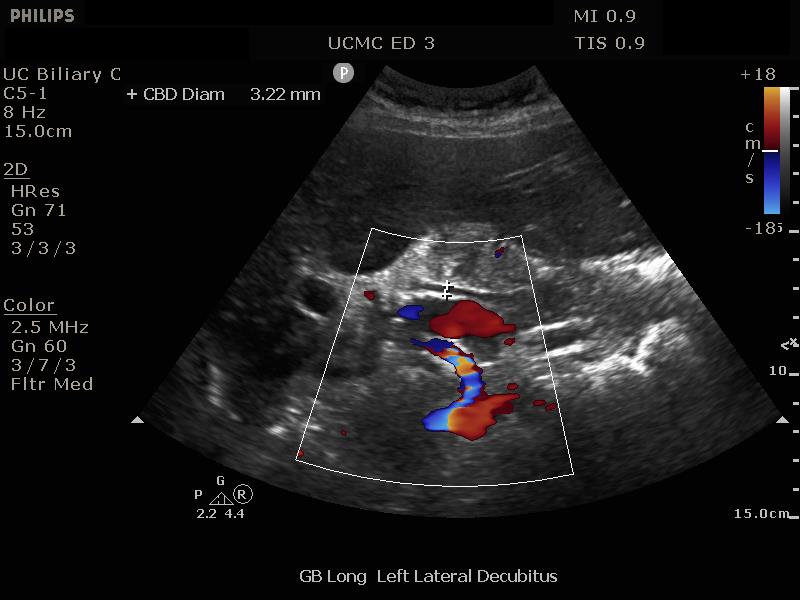
What do you see on ultrasound?
What do you see on ultrasound?
The gallbladder wall is markedly thickened at 7.18 mm (measurement not provided in still images), and there is cholelithiasis. However, none of the stones are in the gallbladder neck or common bile duct (CBD) and there is a normal CBD diameter. There is no pericholecystic fluid. Most notably, while this is not apparent from image reivew, sonographic Murphy’s sign is absent.
Right upper quadrant ultrasound interpretation
Right upper quadrant ultrasound interpretation
In the emergency department the purpose of a focused/limited RUQ ultrasound is to identify signs of cholecystitis, as well as other biliary pathology. The evaluation of the liver parenchyma is unnecessary and beyond the skill set of most providers in the ED. The emergency physician should evaluate for several findings on the RUQ ultrasound1,2:
1) Presence or absence of gallstones. Gallstones are hyperechoic, cause shadowing, and may be seen in the gallbladder or in the common bile duct. While 10-15% of patients in Western populations have gallstones, many of them are asymptomatic, with only obstructive stones (in the neck or the CBD) causing problems3.
2) Gallbladder wall thickness. The gallbladder wall is measured along the anterior wall, preferrably in a section perpendicular to the curvature of the wall. A wall thickness greater than 3 mm is considered abnormal and is a sign of inflammation.
3) Pericholecystic fluid. Identified as hypo- or anechoic material surrounding the gallbladder, not otherwise identifiable as a blood vessel or other organ structure. This is also a sign of gallbladder inflammation.
4) Sonographic Murphy’s sign (SMS). The SMS is defined as maximal tenderness elicited by pressing the gallbladder with the ultrasound probe4,5. When combined with the presence of gallstones, the SMS has been shown to have a sensitivity of 70%, specificity of 77%, positive predictive value of 64% and negative predictive value of 82% in diagnosing cholecystitis4, and is considered to be one of the most important findings on RUQ ultrasound when the differential includes cholecystitis6.
5) Common bile duct dilatation. The commonly accepted upper limit of normal CBD diameter is 6 or 7 mm, with the average diameter around 4 mm. This measurement has been shown to increase with age 8,9. A general rule of thumb is to add 1 mm for every decade of age after 50. A dilated CBD is a sign of biliary obstruction.
GB wall thickening
GB wall thickening
It seems as though the only finding on our patient’s ultrasound that is consistent with cholecystitis is the thickened gallbladder wall. Interestingly, diffuse gallbladder wall thickening is a rather non-specific finding with a wide differential diagnosis that includes cholecystitis, liver disease (hepatitis, cirrhosis, portal venous hypertension), inflammatory states of other adjacent structures (pancreatitis, colitis, pyelonephritis), systemic diseases (congestive heart failure, renal failure, sepsis, hypoproteinemic states), malignancy (gallbladder carcinoma, lymphoma), and adenomyomatosis. “Pseudothickening” can also occur in the postprandial contracted gallbladder9.
Studies have shown that gallbladder wall thickening is frequently seen in patients with viral hepatitis, with an incidence as high as 70%10, and is particularly associated with Hepatitis A 11.
Case Resolution
Case Resolution
The patient’s emergency department providers consulted acute care surgery, who obtained a comprehensive right upper quadrant ultrasound, which was interpreted by our radiologist as follows:
“Diffusely decreased echogenicity of the liver can be seen with hepatitis. Cholelithiasis with gallbladder wall thickening in the absence of a sonographic Murphy's sign is nonspecific in the presence of findings suggestive of hepatitis.”
Considering that our region had recently been experiencing an epidemic of hepatitis A12, a viral serology panel was obtained. The patient was indeed positive for Hepatitis A. She was admitted to the gastroenterology service for symptomatic treatment.
Ultrasound pearls
Ultrasound pearls
- RUQ ultrasound is a focused assessment aiming to shift risk probabilities in patients being evaluted for cholecystitis, biliary colic, cholangitis, and other biliary pathology.
- Gallbladder wall thickening in the absence of other signs of cholecystitis is not particularly specific, and can be seen in pro-inflamamtory states, systemic disorders, and a number of hepatic disease processes.
- Sonographic Murphy's Sign is one of the more predictive signs of cholecystitis when combined with the presence of gallstones.
AUTHORED BY: EMILY ROBLEE, MD
Dr. Roblee is a rising PGY-2 resident in the emergency medicine program at the University of Cincinnati.
PEER REVIEWED BY: PATRICK MINGES, MD
Dr. Minges is an an assistant professor of emergency medicine at the University of Cincinnati and is fellowship trained in Ultrasound.
References
American College of Emergency Physicians. Emergency ultrasound imaging criteria compendium. American College of Emergency Physicians. Annals of emergency medicine. 2006 Oct;48(4):487
Avila J. “Gallbladder.” www.5minsono.com/gb. Accessed 5/26/2019.
Halldestam I, Enell EL, Kullman E, Borch K. Development of symptoms and complications in individuals with asymptomatic gallstones. British journal of surgery. 2004 Jun;91(6):734-8.
Kiewiet JJ, Leeuwenburgh MM, Bipat S, Bossuyt PM, Stoker J, Boermeester MA. A systematic review and meta-analysis of diagnostic performance of imaging in acute cholecystitis. Radiology. 2012 Sep;264(3):708-20.
Bree RL. Further observations on the usefulness of the sonographic Murphy sign in the evaluation of suspected acute cholecystitis. Journal of clinical ultrasound. 1995 Mar;23(3):169-72.
Noble VE, Liteplo AS, Nelson BP, Thomas SH. The impact of analgesia on the diagnostic accuracy of the sonographic Murphy's sign. European Journal of Emergency Medicine. 2010 Apr 1;17(2):80-3.
Perret RS, Sloop GD, Borne JA. Common bile duct measurements in an elderly population. Journal of ultrasound in medicine. 2000 Nov;19(11):727-30.
Park JS, Lee DH, Jeong S, Cho SG. Determination of diameter and angulation of the normal common bile duct using multidetector computed tomography. Gut and liver. 2009 Dec;3(4):306.
Runner GJ, Corwin MT, Siewert B, Eisenberg RL. Gallbladder wall thickening. American Journal of Roentgenology. 2014 Jan;202(1):W1-2.
Ahn JH, Chung JJ, Yu JS, Kim JH, Cho ES, Kim DJ. Prognostic value of gallbladder wall thickening in patients with acute hepatitis A. Ultrasonography. 2015 Apr;34(2):139.
Suk KT, Kim CH, Baik SK, Kim MY, Park DH, Kim KH, Kim JW, Kim HS, Kwon SO, Lee DK, Han KH. Gallbladder wall thickening in patients with acute hepatitis. Journal of Clinical Ultrasound. 2009 Mar;37(3):144-8.
“Hundreds of Hepatitis A Cases in Tri-State.” WCPO, 3 Dec. 2018, www.wcpo.com/news/health/hepatitis-a-outbreak-continues-in-greater-cincinnati-with-hundreds-of-cases.




