Lessons in Transport - Plasma? We Got That...
/
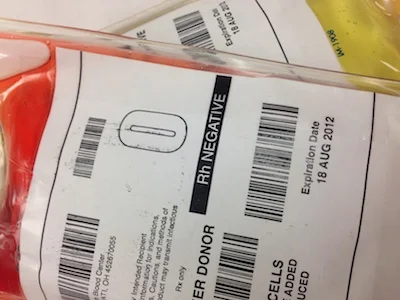
Why is Air Care starting to transport and infuse plasma? Multiple studies, many from military combat zones, strongly suggest that clinical outcomes are improved by administration of plasma alongside RBCs in a 1:1 ratio. (1,2) Furthermore, the concept of damage control resuscitation advocates for minimizing crystalloid infusion and maximizing early aggressive resuscitation with blood products in patients with life threatening hemorrhage. Recent unpublished analysis suggests that expanding these resuscitation principles to the prehospital environment via helicopter EMS was associated with improved outcomes.
Read More