A Finger on the Pulse or An Ultrasound Probe on the Pulse?
/Cohen, A. L. et al. Femoral artery Doppler ultrasound is more accurate than manual palpation for pulse detection in cardiac arrest. Resuscitation 173, 156–165.
Background

Data has shown that manual palpation of pulse checks is limited by body habitus, environmental stress, time limitations, and assessor experience; thereby limiting the accuracy of manual pulse detection which varies from 63% to 94%. This study set out to assess the accuracy of femoral artery doppler ultrasound compared to manual palpation to detect a pulse in patients in cardiac arrest. Their secondary objective was to determine whether peak systolic velocity (PSV) on doppler ultrasound could accurately detect a pulse with an adequate blood pressure needed for perfusion, which was defined as SBP ≥ 60 mmHg.
Methods
This study was a prospective, cross-sectional, partially blinded, diagnostic accuracy study performed in a quaternary care Emergency Department (ED) between June 2019 to July 2021.
The patients included were adults ≥ 18 years old with nontraumatic cardiac arrest. They needed to have an arterial line placed and a Doppler ultrasound-trained Emergency Medicine attending needed to be available. Patients were excluded if they were a candidate for extracorporeal membrane oxygenation (ECMO).
At each pulse check, research personnel confirmed and recorded whether; the treatment team palpated a pulse, the presence or absence of a doppler ultrasound signal, the arterial line waveforms and highest SBP on the arterial line, and the highest PSV on ultrasound.
Outcomes and Results
A total of 54 patients and 213 pulse checks were included for the primary outcome detection of any pulse. The patients were mostly elderly white males, predominantly in non-shockable rhythms.
Doppler ultrasound had higher accuracy than manual palpation for detection of any pulse (95.3% vs. 54.0%; p < 0.001).
When SBP ≥ 60 mmHg, the accuracy of Doppler ultrasound was lower, however still more accurate than manual palpation (77.6% vs. 66.2%; p = 0.011)
When SBP ≥ 60 mmHg, the sensitivity of manual palpation was low at 47.4%; however, the specificity of manual palpation was higher than Doppler ultrasound (82.3% vs. 58.4%; p < 0.001).
The optimal cut-off value for PSV associated with a SBP ≥ 60 mmHg was 20 cm/s. To detect SBP ≥ 60 mmHg, the accuracy of PSV ≥ 20 cm/s on Doppler ultrasound was higher than manual palpation (91.4% vs. 66.2%; p < 0.001).
Limitations
The study was a single-center study with a small number of patients and was terminated early due to an interim analysis that favored ultrasound use over manual palpation. In addition, treatment teams were not blinded to the arterial line waveforms. This study did not evaluate clinical outcomes based on differences in the method of pulse check.
Conclusions
This study showed that femoral artery Doppler ultrasound was significantly more accurate than manual palpation for detecting any pulse, but less specific for a SBP > 60. However, a PSV ≥ 20 cm/st was found to predict a pulse with a SBP ≥ 60 mmHg, which was considered adequate for perfusion.

How to utilize power doppler to find the femoral pulse using ultrasound
Chose a linear probe, in vascular setting
Find your anatomy
Select power doppler and place the marker in the artery
Click power doppler again for the flow
Utilize your baseline and scale to make adjustments so you can see the entirety of the forward flow velocities

Image 1. Right femoral region with the femoral artery and vein displayed

Image 2. Choose power doppler (PW) seen in the yellow box and select it again once the marker is in the middle of the vessel. Use the baseline and scale buttons to optimize your image
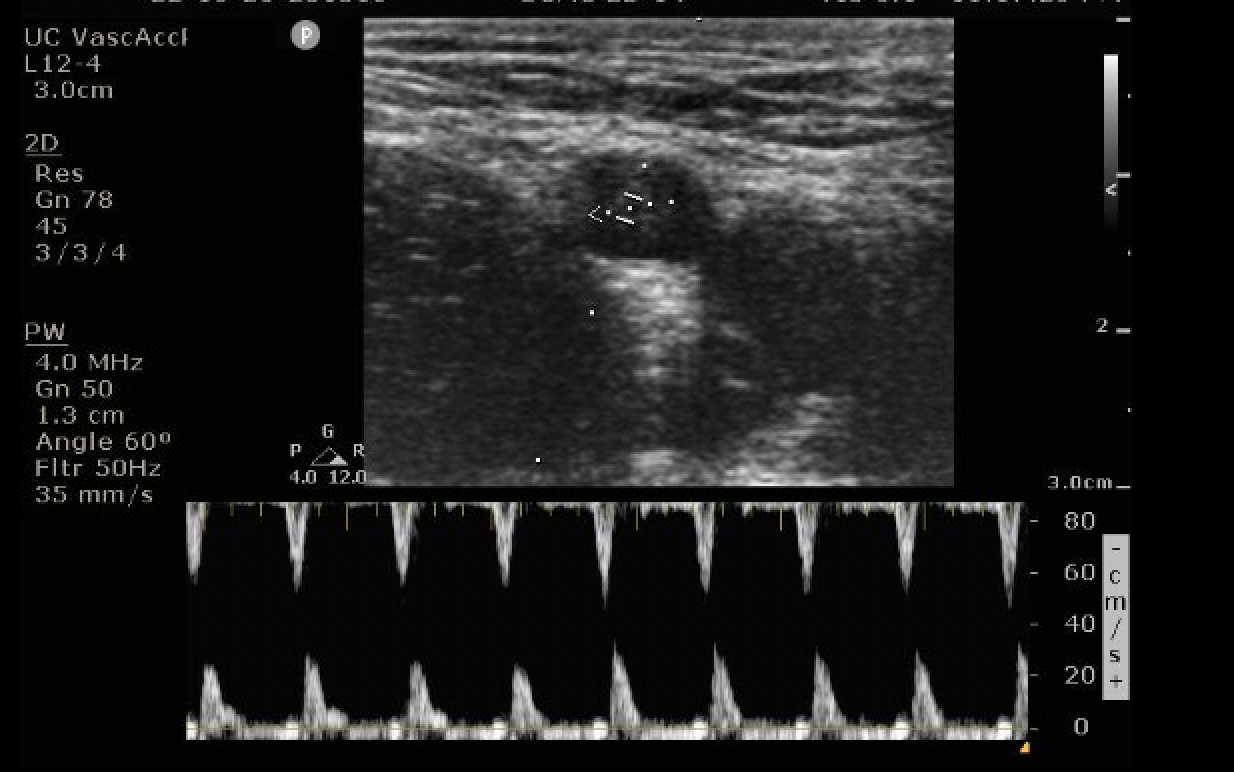
Image 3. Cursor through the femoral artery. Peak systolic velocity (PSV) scale on the right. Max PSV > 20 cm/s
Authorship
Written by - Martina Diaz, MD, PGY-3, University of Cincinnati Department of Emergency Medicine
Peer Review - Patrick Minges, MD
Peer Review, Editing, Posting - Jeffery Hill, MD MEd
Cite As
Diaz, M. Minges, P., Hill, J. (November 4, 2022) A Finger on the Pulse or An Ultrasound Probe on the Pulse? TamingtheSRU. https://www.tamingthesru.com/blog/2022/11/2/pulse-checks




